Can torsades de pointes have a pulse

Andrew Campbell
Published Mar 10, 2026
Patients with torsade may be hypotensive, have a rapid pulse and have loss of consciousness.
What is the heart rate in Torsades de Pointes?
Unlike a normal pulse rate of 60 to 100 beats a minute, a fast heartbeat in your ventricles (ventricular tachycardia) is more than 100 beats a minute. Torsades de Pointes can lead to a heart rate anywhere between 150 to 300 beats a minute.
Do you do CPR for torsades de pointes?
Consider magnesium for torsades de pointes associated with a long QT interval (see below). You should administer the drug during CPR, as soon as possible after rhythm analysis. If a nonshockable rhythm is present and the rhythm is organized (complexes appear regular or narrow), try to palpate a pulse (see Box 12).
What are the characteristics of torsades de pointes?
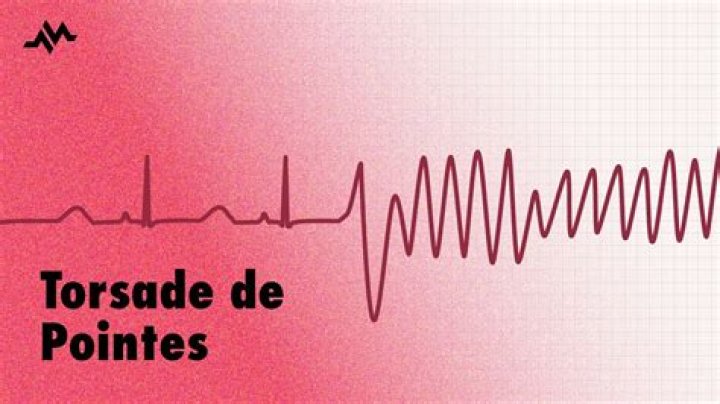
Torsades de pointes is a specific form of polymorphic ventricular tachycardia in patients with a long QT interval. It is characterized by rapid, irregular QRS complexes, which appear to be twisting around the electrocardiogram (ECG) baseline.Is torsades de pointes VT or VF?
Frequent PVCs with ‘R on T’ phenomenon trigger a run of polymorphic VT which subsequently begins degenerates into VF. QT interval is difficult to see because of artefact but appears slightly prolonged (QTc ~480ms), making this likely to be TdP.
What is the cause of Torsades de Pointes?
Common causes for torsades de pointes include drug-induced QT prolongation and less often diarrhea, low serum magnesium, and low serum potassium or congenital long QT syndrome. It can be seen in malnourished individuals and chronic alcoholics, due to a deficiency in potassium and/or magnesium.
Does Idioventricular rhythm have a pulse?
An idioventricular rhythm — not accelerated — has a heart rate of < 60 beats per minute. AIVR is hemodynamically stable, and thus no specific treatment is needed.
Why does prolonged QT cause tachycardia?
Long QT syndrome (LQTS) is caused by malfunction of cardiac ion channels impairing ventricular repolarization. This predisposes to the development of the polymorphic ventricular tachycardia torsade de pointes (‘twisting of the points’) (Fig. 1).What is the heart doing in torsades?
A: Torsades de pointes is a ventricular tachycardia, meaning that it is a fast heartbeat with the electrical activity from the ventricles. The ventricles are the two lower chambers of the heart that pump blood first from the right side of the heart to the lungs, and then from the left side out to the rest of the body.
Is amiodarone contraindicated in torsades?Torsades de pointes is caused by a prolonged QT. Almost all of the antiarrhythmics that we normally use to treat ventricular tachycardia, such as amiodarone and procainamide, will prolong the QT further, and therefore can make your patient worse. Do not give amiodarone or procainamide.
Article first time published onWill AED shock torsades?
Conclusion: Lay-rescuer AEDs and professional hospital defibrillators tested in AED mode did not reliably recommend a shock for sustained monomorphic VT or TdP at certain rates, despite the fact that it is a critical component of the currently recommended treatment.
How do you treat torsades de pointes?
Treatment of torsade de pointes includes: isoproterenol infusion, cardiac pacing, and intravenous atropine. Intravenous magnesium sulfate, a relatively new mode of therapy for torsade de pointes, was proven to be extremely effective and is now regarded as the treatment of choice for this arrhythmia.
How can you tell Torsades de Pointes?
- heart palpitations.
- dizziness.
- nausea.
- cold sweats.
- chest pain.
- shortness of breath.
- rapid pulse.
- low blood pressure.
Do you shock VT with a pulse?
Under current resuscitation guidelines symptomatic ventricular tachycardia (VT) with a palpable pulse is treated with synchronised cardioversion to avoid inducing ventricular fibrillation (VF), whilst pulseless VT is treated as VF with rapid administration of full defibrillation energy unsynchronised shocks.
What is the difference between Torsades and polymorphic VT?
Polymorphic VT is defined as an unstable rhythm with a continuously varying QRS complex morphology in any recorded ECG lead. Polymorphic VT that occurs in the setting of QT prolongation is considered as a distinct arrhythmia, known as torsades de pointes.
Do you defibrillate v tach with a pulse?
Ventricular tachycardia is a poorly perfusing rhythm; patients may present with or without a pulse. Most patients with this rhythm are unconscious and pulseless and defibrillation is needed to “reset” the heart so that the primary pacemaker (usually the Sinoatrial Node) can take over.
Can you do CPR on asystole?
Asystole is treated by cardiopulmonary resuscitation (CPR) combined with an intravenous vasopressor such as epinephrine (a.k.a. adrenaline). Sometimes an underlying reversible cause can be detected and treated (the so-called “Hs and Ts”, an example of which is hypokalaemia).
Is junctional tachycardia a ventricular rhythm?
If the QRS complex is wide, an accelerated junctional rhythm resembles an accelerated ventricular rhythm. The rate of the ectopic ventricular rhythm is usually 70 to 110 beats/min.
What happens to the heart during Idioventricular rhythm?
Idioventricular rhythm: An independent pacemaker in the ventricles discharging at a relatively slow rate, dominating the cardiac rhythm, resulting in a normal or almost normal heart rate.
Which drug is associated with torsades de pointes?
Antiarrhythmic drugs associated with torsade include the following: Class IA – Quinidine, disopyramide, procainamide. Class III – Sotalol, amiodarone (rare), ibutilide, dofetilide, almokalant.
Who is at risk for torsades de pointes?
Risk factors for torsade include the following: Congenital long QT syndrome. Female gender. Acquired long QT syndrome (causes of which include medications and electrolyte disorders such as hypokalemia and hypomagnesemia)
What medications can cause torsades?
Other drugs that prolong the QT interval and have been implicated in cases of torsade include phenothiazines, tricyclic antidepressants, lithium carbonate, ziprasidone, cisapride, highly active antiretroviral drugs, high-dose methadone, anthracycline chemotherapeutic agents (eg, doxorubicin, daunomycin), some …
Can prolonged QT cause torsades?
In LQTS, QT prolongation can lead to polymorphic ventricular tachycardia, or torsade de pointes, which itself may lead to ventricular fibrillation and sudden cardiac death.
Does Long QT always show on ECG?
EKG (Electrocardiogram) Not all people who have LQTS will always have a long QT interval on an EKG. The QT interval may change from time to time; it may be long sometimes and normal at other times. Thus, your doctor may want you to have several EKG tests over a period of days or weeks.
Does polymorphic ventricular tachycardia have a pulse?
Q: What sort of a pulse would you be feeling with a polymorphic VT? A: You may feel a weak pulse or a strong pulse depending on how long the polymorphic VT has been going on.
Can you get torsades with a pacemaker?
Torsades de pointes tachycardia may be triggered by several factors, including antiarrhythmic drugs, hypokalaemia, and acquired or congenital long QT syndrome. Asynchrony or faulty pacemaker activity may also, although very rarely, be associated with torsades de pointes.
What heart rhythms are shockable?
The two shockable rhythms are ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT) while the non–shockable rhythms include sinus rhythm (SR), supraventricular tachycardia (SVT), premature ventricualr contraction (PVC), atrial fibrilation (AF) and so on.
Does procainamide cause torsades?
Drugs in a number of drug classes have been associated with torsade. Antiarrhythmic drugs associated with torsade include the following: Class IA – Quinidine, disopyramide, procainamide.
How does magnesium work in Torsades de Pointes?
Magnesium is the drug of choice for suppressing early afterdepolarizations (EADs) and terminating the arrhythmia. Magnesium achieves this by decreasing the influx of calcium, thus lowering the amplitude of EADs. Magnesium can be given at 1-2 g IV initially in 30-60 seconds, which then can be repeated in 5-15 minutes.
How is VT diagnosed on ECG?
Frequently, this is difficult to see due to the fast rate of the QRS complex. Below is an ECG strip of a patient with VT. See the PP interval when in sinus rhythm then march out the P waves within the wide QRS complex to find the AV dissociation that is present, confirming the diagnosis of VT.
Does Epi prolong QT?
Conclusions: Epinephrine-induced prolongation of the QT interval appears pathognomonic for LQT1. Low-dose epinephrine infusion distinguishes controls from patients with concealed LQT1 manifesting an equivocal QTc at rest.