How do you write a nursing sbar

Andrew Campbell
Published Mar 05, 2026
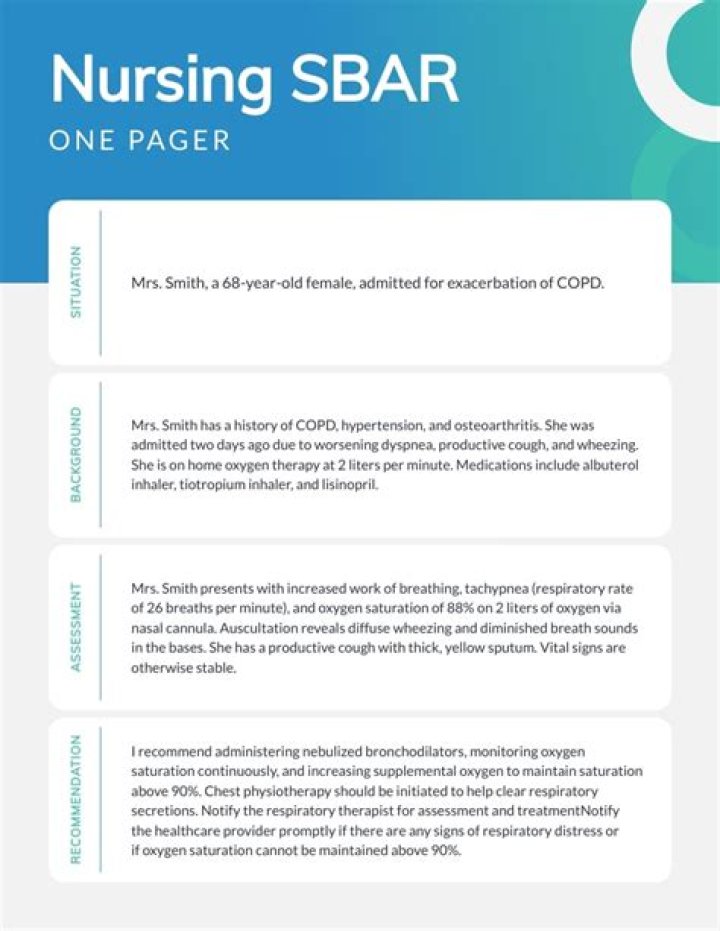
Situation: Clearly and briefly describe the current situation.Background: Provide clear, relevant background information on the patient.Assessment: State your professional conclusion, based on the situation and background.
What are examples of SBAR?
- Nurse-to-provider communication. Used to help the nurse when calling to report a patient’s deteriorating condition or requesting something for the patient.
- Nurse-to-Nurse or other nursing staff. during transfers to other units or patient report hand-offs.
What is the first step of SBAR?
Each component of SBAR—situation, background, assess- ment, recommendation—provides a format for which to present information in a specific, organized way. The first step of the SBAR tool is stating the situation. In other words, what is the problem?
What is the SBAR format in nursing?
The SBAR (Situation-Background-Assessment-Recommendation) technique provides a framework for communication between members of the health care team about a patient’s condition.What does SBAR stand for and what is an example?
Communicating with SBAR. The SBAR (situation, background, assessment and recommendation) tool is provided below to aid in facilitating and strengthening communication between nurses and prescribers throughout the implementation of this quality improvement initiative.
What is an SBAR handover?
The communication tool SBAR (situation, background, assessment and recommendation) was developed to increase handover quality and is widely assumed to increase patient safety. … Primary and secondary outcome measures Aspects of patient safety (patient outcomes) defined as the occurrence or incidence of adverse events.
How do I create an SBAR file?
- Situation: Clearly and briefly describe the current situation.
- Background: Provide clear, relevant background information on the patient.
- Assessment: State your professional conclusion, based on the situation and background.
What does SOAP stand for?
Introduction. The Subjective, Objective, Assessment and Plan (SOAP) note is an acronym representing a widely used method of documentation for healthcare providers.How long should an SBAR be?
It is recommended that this element be brief and last no more than 10 seconds. It is recommended that health care professionals identify the person with whom they are speaking, to introduce oneself (including title or role) and where one is calling from.
Why do nurses use sbar?SBAR technique has helped nurses to have a focused and easy communication during transition of care during handover. … Use of standardized SBAR in nursing practice for bedside shift handover will improve communication between nurses and thus ensure patient safety.
Article first time published onWhat should the nurse do if an abnormal finding has been assessed?
If any abnormal findings are identified, the nurse must ensure that appropriate action is taken. This may include communicating the findings to the medical team, relevant allied health team and the ANUM in charge of the shift.
When should a nurse use sbar?
- Conversations with physicians, physical therapists, or other professionals.
- In-person discussions and phone calls.
- Shift change or handoff communications.
- When resolving a patient issue.
- Daily safety briefings.
- When you’re escalating a concern.
- When calling an emergency response team.
Which behaviors help patients develop trust in the nurse?
Showing respect and caring Being compassionate, spending appropriate time with patients, demonstrating active listening, and helping to advise and resolve the patient’s problems will all contribute to building a trusting, respectful relationship.
In which scenario would the nurse give a verbal report to another healthcare professional?
In which scenario would the nurse give a verbal report to another healthcare professional? d. the nurse is going home at the end of his shift – Whenever a patient is transferred from one person’s care to another, the original worker must give a verbal report.
Which of the following words is a component of sbar?
Using SBAR (Situation, Background, Assessment, and Recommendation) communication, which of the following is the correct order? a.
How do I write a good bedside report?
- Give a Bedside Report. “Check pertinent things together such as skin, neuro, pulses, etc. …
- Be Specific, Concise and Clear. “Stay on point with the ‘need to know’ information. …
- When in Doubt, Ask for Clarification. …
- Record Everything. …
- Be Positive!
What type of writing is done in nursing?
Clinical nurses write book chapters, books, and journal articles for publication. Written communication is one way that information about the practice of nursing is disseminated with others. Nurses in management write reports, proposals, reference letters, human resource reports, and staff performance appraisals.
How do you start a report?
- Decide on terms of reference.
- Conduct your research.
- Write an outline.
- Write a first draft.
- Analyze data and record findings.
- Recommend a course of action.
- Edit and distribute.
How do you write a soapie note?
- Summarize subjective information. Record subjective information about the patient’s experience in the first section of the SOAPIE note. …
- List objective data. …
- Complete a patient assessment. …
- Outline the treatment plan. …
- Describe healthcare interventions. …
- Evaluate the interaction.
What is cus in nursing?
Concerned, Uncomfortable, Safety (a communication tool for nurses used to convey to physicians important changes in the health status of patients).
What does sbar stand for quizlet?
Situation, Background, Assessment, Recommendation.
What should a nursing handover include?
- Past: historical info. The patient’s diagnosis, anything the team needs to know about them and their treatment plan. …
- Present: current presentation. …
- Future: what is still to be done.
How do I write an iSoBAR?
The acronym “iSoBAR” (identify–situation–observations–background–agreed plan–read back) summarises the components of the checklist.
What should be included in sbar handover?
Identify yourself and the site/unit you are calling from • Identify the patient by name and the reason for your report • Describe your concern. Firstly, describe the specific situation about which you are calling, including the patient’s name, consultant, patient location, resuscitation status and vital signs.
What are the disadvantages of sbar?
Limitations of SBAR tool The SBAR tool requires training of all clinical staff so that communication is well understood. It requires a culture change to adopt and sustain structured communication formats by all health care providers.
What does the abbreviation SX mean in medical terms?
Dx – Diagnosis, Sx – Symptoms, Fx – Fracture, Tx – Treatment, Hx – History S/b-seen by. Sortable table. Abbreviation. Meaning.
What goes in the assessment part of a SOAP note?
An assessment is the diagnosis or condition the patient has. In some instances, there may be one clear diagnosis. In other cases, a patient may have several things wrong. … Plan: The last section of a SOAP note is the plan, which refers to how you are going to address the patient’s problem.
What is foaming capacity of soaps?
When soap is shaken with water it becomes a soap solution that is colloidal in nature. Agitating it tends to concentrate the solution on the surface and causes foaming. This helps the soap molecules make a unimolecular film on the surface of water and to penetrate the fabric.
Which of the following statements describes the purpose of the nursing process?
Which of the following statements describes the purpose of the nursing process? … The nursing process is a way to systematically think about and use patient data.
What are five rights of delegation?
Utilize the five rights of delegation (e.g., right task, right circumstances, right person, right direction or communication, right supervision or feedback) Evaluate delegated tasks to ensure correct completion of activity.
How do you document skin turgor?
They main way to test skin turgor is to lightly pinch your skin, usually on your arm or abdomen. If it takes longer than usual for the skin to bounce back, it could be a sign of dehydration.