Is Lcis a cancer

Andrew White
Published Mar 13, 2026
LCIS is not considered to be cancer, and it typically does not spread beyond the lobule (become invasive breast cancer) if it isn’t treated. But having LCIS does increase your risk of developing an invasive breast cancer in either breast later on, so close follow-up is important.
How often does LCIS turn into cancer?
The risk of breast cancer in women diagnosed with LCIS is thought to be approximately 20 percent. Put another way, for every 100 women diagnosed with LCIS , 20 will be diagnosed with breast cancer and 80 won’t be diagnosed with breast cancer.
Can LCIS be removed?
The best way to treat LCIS found on a needle biopsy is not clear. In some cases where LCIS is found on needle biopsy, the doctor might recommend that it be removed completely (with an excisional biopsy or some other type of breast-conserving surgery).
Which is worse LCIS or DCIS?
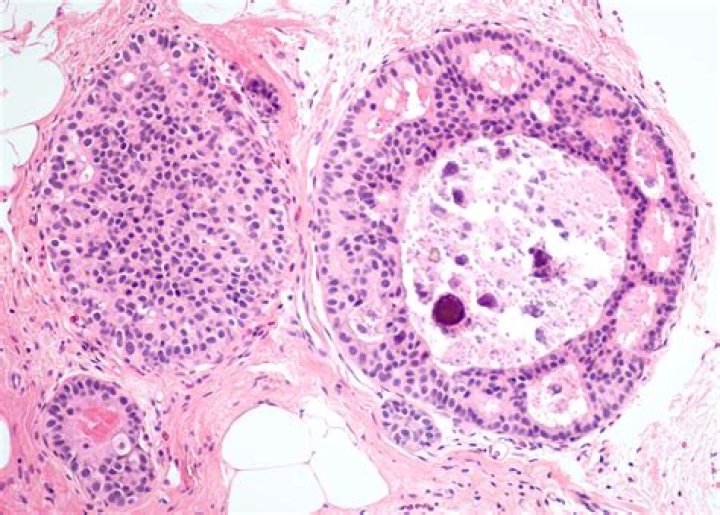
Lobular Carcinoma In Situ. Lobular Carcinoma in Situ (LCIS) is a malignancy of the secretory lobules of the breast that is contained within the basement membrane (Fig. 3). They are much rarer than DCIS however individuals with LCIS are at greater risk of developing an invasive breast malignancy.Is LCIS high risk?
Proliferative lesions with atypia include atypical ductal hyperplasia (ADH), atypical lobular hyperplasia (ALH), and lobular carcinoma in situ (LCIS). These lesions are considered high risk because they are associated with an increase in the patient’s future risk of developing breast cancer [1].
How long does it take for LCIS to become invasive?
If a woman with LCIS develops an invasive breast cancer, it doesn’t typically happen within a few years. Rather, it is more likely to happen over the long-term — in 10, 15, or 20 years or even beyond that.
Should I worry about LCIS?
LCIS is not considered to be cancer, and it typically does not spread beyond the lobule (become invasive breast cancer) if it isn’t treated. But having LCIS does increase your risk of developing an invasive breast cancer in either breast later on, so close follow-up is important.
Does LCIS show up on MRI?
Lobular carcinoma in situ (LCIS) is a nonmalignant, proliferative condition that is a marker for an increased risk of breast malignancy. It is usually indistinguishable from benign parenchyma on MRI.Should LCIS be excised?
Conclusion: Excision is recommended for LCIS on core biopsy because of its 8.4-9.3% upgrade rate. Excluding discordant cases, patients with other high-risk lesions or concurrent malignancy, the risk of upgrade of ALH was 2.4%.
Does LCIS need radiation?LCIS does not require treatment in the way you might normally think of cancer treatment, such as needing to have surgery, radiation therapy, and chemotherapy. You and your doctor may decide that you should undergo careful observation to watch for any signs of invasive breast cancer.
Article first time published onHow rare is LCIS?
LCIS is usually diagnosed before menopause, most often between the ages of 40 and 50. Less than 10% of women diagnosed with LCIS have already gone through menopause. LCIS is extremely uncommon in men. LCIS is viewed as an uncommon condition, but we don’t know exactly how many people are affected.
Should I get a double mastectomy for LCIS?
Current guidelines recommend counseling on risk reduction strategies, including lifestyles modification, endocrine therapy, and bilateral mastectomy, for patients with classic-type LCIS detected on core biopsy or surgical excision.
What percentage of LCIS becomes invasive?
109 (65%) of the cancers were invasive — 85% of these cancers were hormone-receptor-positive. 59 (35%) of the cancers were DCIS.
Is invasive lobular carcinoma fast growing?
Invasive lobular carcinoma grades The lowest — grade 1 — refers to cancer cells that resemble normal breast cells, are slow-growing, and least likely to spread. Grade 2 cells look less like normal cells and are growing a bit faster. Grade 3 cells look much different and will likely grow and spread the fastest.
Does LCIS need excisional biopsy?
CNB findingExcisional biopsy recommendationClassic LCIS with concordant imagingConsider excisionClassic LCIS identified on MRIRecommended
Is ALH a high risk lesion?
ADH is considered a pre-malignant, high-risk lesion, and ALH only a high-risk lesion. Either can be found in association with or at the periphery of a more advanced lesion; therefore, it is important to remember that atypical hyperplasia found on a biopsy may not accurately represent the greater lesion.
What stage is lobular carcinoma in situ?
Stage 0 means the cancer cells are still within the breast lobule and have not invaded deeper into the surrounding fatty breast tissue. This is called lobular carcinoma in situ (LCIS), a non-invasive breast cancer. In stage 0 cancer, the cancer has not spread to lymph nodes or distant sites.
What is LCIS classic type?
Classic LCIS is a monomorphic, dyshesive proliferation of non-polarized cells with round to oval shape, inconspicuous cytoplasm. The nuclei are located in the center of the cells, and are small, round to oval, with smooth nuclear membrane and inconspicuous nucleoli (Fig. 3). Cell borders are indistinct.
Should I take tamoxifen for LCIS?
It’s strongly recommended women with LCIS take tamoxifen or raloxifene to lower their risk of breast cancer [188]. Both tamoxifen and raloxifene can lower the risk of [235]: Invasive breast cancer. Non-invasive breast cancers, such as ductal carcinoma in situ (DCIS)
How often is LCIS bilateral?
Lobular carcinoma-in-situ (LCIS) LCIS comprises 30–50% of carcinoma-in-situ, associated with invasive cancer in 10% and are frequently bilateral (35–60%).
What does LCIS look like on a mammogram?
Symptoms of LCIS On a mammogram, microcalcifications show up as white specks. It’s believed that many cases of LCIS simply go undiagnosed, and they may never cause any problems.
Why are lobular cancers sneaky?
Instead of clustering together, lobular cells spread out single file like tree branches or spider webs or mesh, which explains why surgeons and oncologists often refer to it as “sneaky” or “insidious.” Because the cells don’t stick together well, there’s often no lump, making it harder for women to find during self- …