Where is residual volume trapped

Sarah Rodriguez
Published Mar 08, 2026
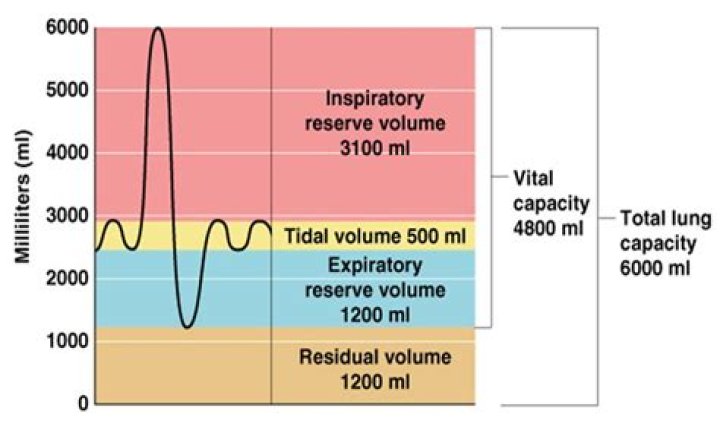
Residual volume (RV) is the volume of air remaining in the lungs after maximum forceful expiration. In other words, it is the volume of air that cannot be expelled, thus causing the alveoli to remain open at all times.
How do you find the residual volume of a lung?
*RV is the volume that remains in the lungs after maximal expiration. (Also, RV= TLC-VC).
Why is there always residual volume left in the lungs?
Why Do We Need Residual Volume? The lungs are never completely empty; there is always some air left in the lungs after a maximal exhalation. The air that remains in the lungs is needed to help keep the lungs from collapsing. … Residual volume is necessary for breathing and proper lung function.
Is residual volume dead space?
Hint: No, residual volume and dead space volume are not synonymous. Residual volume is a normal phenomenon but the dead space volume(physiological dead space) occurs due to lack of the blood supply into the alveoli resulting in the improper gaseous exchange of the alveoli.What happens to residual volume as you age?
Functional residual capacity and residual volume increase with age, resulting in a lower vital capacity. Gas exchange in the lungs occurs across the alveolar capillary membrane.
What is IC in respiratory?
Inspiratory Capacity (IC) is the amount of air that can be inhaled after passive expiration. It is the sum of the IRV and the VT. Vital Capacity (VC) is the amount of air that can move in and out of the lungs.
Where is anatomic dead space?
Anatomic dead space specifically refers to the volume of air located in the respiratory tract segments that are responsible for conducting air to the alveoli and respiratory bronchioles but do not take part in the process of gas exchange itself.
Is PE shunt or dead space?
Pulmonary embolism (PE) is an example of increased dead space resulted in decreasing perfusion relative to ventilation. Shunt and dead space are two conditions of lungs, resulting in impaired gas exchange. Moreover, they are examples of the ventilation-perfusion (V/Q) mismatch.When summed with Erv is called?
Inspiratory Capacity (IC): Sum of the tidal volume plus the inspiratory reserve volume (TV + IRV). … This value includes the expiratory reserve volume plus the residual volume (ERV + RV). Vital Capacity (VC): Vital capacity is the total usable volume of the lungs which is under voluntary control.
Why would a patient have a high residual volume?Increased lung volumes, particularly residual volume (RV), are commonly observed in airway obstruction. TLC may be normal, but is frequently increased in the late stages of COPD. Hyperinflation and air-trapping are terms commonly used to reflect these changes, but are not well standardized.
Article first time published onWhat happens to residual volume after death?
If the lungs sink, no residual air remains, so it is likely the person drowned after inhaling large amounts of water. However, if the lungs float, the residual volume of air remains in the lungs. The residual volume was not replaced by water, so it is likely the person died before entering the water.
What is the residual volume of lungs Class 10?
The residual volume is about the total volume of air around 1100 ml to 1200 ml residing in the lungs after the reserve volume is emitted or breathed out.
How does COPD affect residual volume?
This is also called the resting volume. Loss of lung elasticity due to emphysema in COPD reduces the lung recoil pressure. Consequently, FRC or resting volume occurs at a higher volume, which defines static hyperinflation (short-dashed lines).
How can I test my lung capacity at home?
- Set the pointer. …
- Attach the mouthpiece to the meter. …
- Sit up or stand up as straight as you can, and take a deep breath.
- Close your lips tightly around the mouthpiece. …
- Breathe out as hard and as fast as you can for 1 or 2 seconds. …
- Write down the number on the gauge. …
- Repeat these steps 2 more times.
What is destroyed in emphysema?
Emphysema develops over time and involves the gradual damage of lung tissue, specifically the destruction of the alveoli (tiny air sacs). Gradually, this damage causes the air sacs to rupture and create one big air pocket instead of many small ones.
What decreases dead space?
Sleep: Anatomic dead space is believed to decrease during sleep and be the primary physiologic cause of observed decreases in tidal volume, minute ventilation, and respiratory rate during sleep. Maxilla: Variation also can occur in patients with maxillary defects or those who have undergone maxillectomy procedures.
Does dead space cause hypercapnia?
Nonetheless, energy is required to ventilate the physiological dead space, although neither oxygen gain nor carbon dioxide removal occurs. … Beyond that point, inadequate ventilation caused by extensive physiological dead space can lead to acute respiratory failure of the hypercapnic variety.
What happens when you increase anatomical dead space?
Increasing the alveolar dead space with a normal anatomical/apparatus component will increase your minute volume requirements proportionally to the change in the rato of dead space to alveolar ventilation.
What are the 4 lung volumes?
Four standard lung volumes, namely, tidal (TV), inspiratory reserve (IRV), expiratory reserve (ERV), and residual volumes (RV) are described in the literature. Alternatively, the standard lung capacities are inspiratory (IC), functional residual (FRC), vital (VC) and total lung capacities (TLC).
When 1200 mL air is left in the lungs it is called?
Residual Volume (RV): Volume of air remaining in the lungs even after a forcible expiration. This averages 1100 mL to 1200 mL.
What happens to TLC and VC in fibrosis?
VC per se is not a useful indicator for differential diagnosis, because it decreases in both obstructive and restrictive lung disorders such as atelectasis and pulmonary fibrosis. TLC, on the other hand, is decreased in restrictive disease but is increased by air trapping in obstructive disorders.
What is IC in lung capacity?
IC is a lung volume that is captured during a pulmonary function test, which can be used to determine the mechanical function of your lungs. Inspiratory capacity is measured as you exhale casually followed by a maximal inhalation. 1 The normal inspiratory capacity in an adult is approximately 3 liters.
What is IC in spirometry?
The significance of measuring inspiratory capacity (IC) during forced spirometry in cystic fibrosis is vague. A reduction in IC may be noted in the presence of hyper- inflation and trapped air, frequently accompanied by dyspnea due to breathing at high lung volumes.
What do low lung volumes mean?
Low lung volume If your lung volume is lower than normal, this may be a sign of a restrictive lung condition such as pulmonary fibrosis or sarcoidosis.
What is the purpose of residual volume?
Residual volume is the amount of air that remains in a person’s lungs after fully exhaling. Doctors use tests to measure a person’s residual air volume to help check how well the lungs are functioning.
What is the difference between functional residual volume and residual volume?
Tidal volumeResidual VolumeApproximately it measures around 500 ml of air in a healthy adult man.Approximately it measures around 1100-1200 ml of air in a healthy adult man.
What damages brain damage persists longer than 4 to 6 minutes?
Another significant cause of brain injury is a lack of oxygen to the brain. Known as anoxic brain injuries or hypoxic brain injuries, these afflictions result from oxygen deprivation that lasts more than a few minutes.
Is atelectasis a shunt or V Q mismatch?
The major cause of this derangement is shunt, an effect of prompt atelectasis formation in dependent lung regions. An additional cause is ventilation/perfusion (V/Q) mismatch, possibly produced by intermittent airway closure.
Does PE improve with oxygen?
Treatment goals for pulmonary embolism are to improve oxygenation and cardiac output. Administer supplemental oxygen via nasal cannula or non-rebreather mask to maintain SPO2 above 94 percent. Be aware that reduced blood flow to the lungs may prevent improvement of hypoxia from oxygen administration.
What is VQ mismatch vs shunt?
When the proper balance is lost between ventilated alveoli and good blood flow through the lungs, ventilation perfusion mismatch is said to exist. The ventilation/perfusion ratio is often abbreviated V/Q. … Shunt is perfusion of poorly ventilated alveoli. Physiologic dead space is ventilation of poor perfused alveoli.
How is residual volume affected?
Residual volume is determined by competing factors: the strength of the expiratory muscles and the inwards pull of the lungs tending to decrease residual volume, and the outward pull of the chest wall tending to increase residual volume.